
Overview

Visit our COVID-19 website for more information
For more information about the 2026 Influenza Immunisation Programme, click here
To view or download the 2026 Winter Preparedness Kit (formerly the Flu Kit), please click here
Annual influenza immunisation is recommended to provide protection from the predominant circulating influenza strains. The vaccine should be given before the influenza season in New Zealand.
The World Health Organization monitors influenza illness throughout the year and makes recommendations on which influenza types are likely to cause the most illness in the northern and in the southern hemisphere during their respective influenza seasons. Vaccine ingredients are specific to the brand of influenza vaccine they are associated with and may vary to year. Specific information on ingredients in the vaccines use each season can be found in the individual Medsafe vaccine datasheets.
Influenza vaccinations are available funded to the eligible population. Click here for details on eligibility.
Those not eligible for funded influenza vaccinations can purchase through their family doctor or community pharmacy.
Some employers fund influenza vaccinations for their employees.
Influenza vaccine 2026 strains
In 2026, the Southern Hemisphere egg-based and cell culture vaccines contain different strains, as recommended by the WHO.
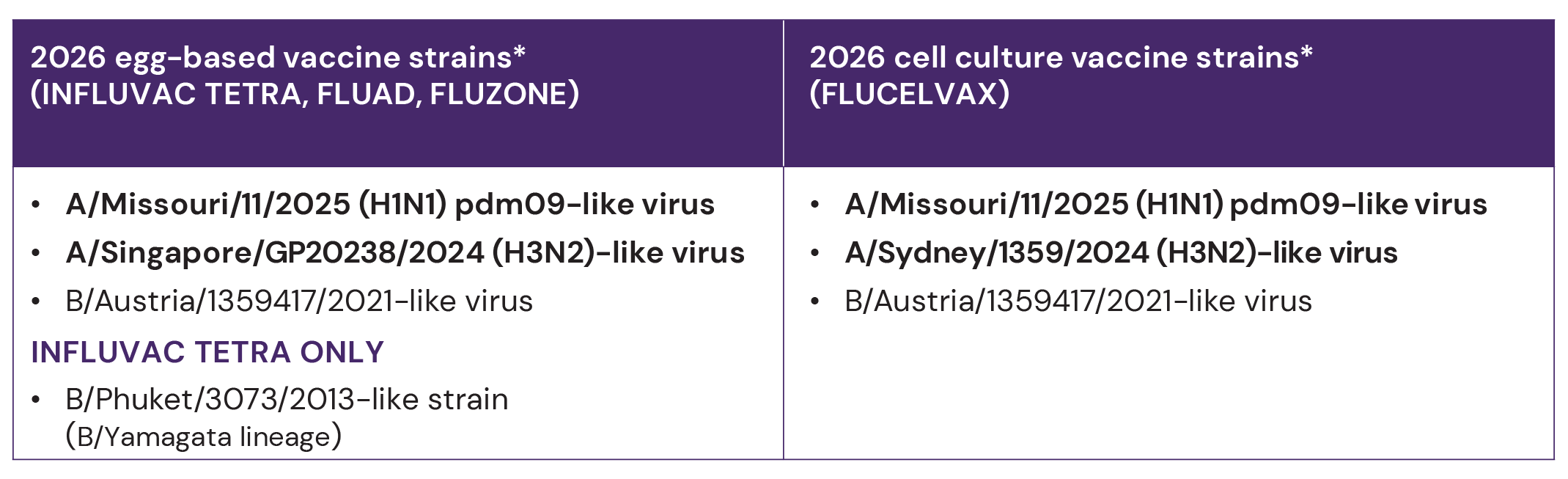
* Bolded strains are new for 2026
Trivalent and quadrivalent vaccine options
The 2026 funded vaccine Influvac Tetra remains a quadrivalent vaccine that protects against four different influenza strains, while the unfunded vaccine options have shifted to trivalent formulations and do not include the B/Yamagata strain. Protection against this strain is no longer considered necessary by WHO as B/Yamagata strains have not been detected since 2020. In the current context, both the trivalent and quadrivalent vaccines are expected to provide equal levels of protection for consumers. The absence or presence of the fourth strain does not impact on the safety or effectiveness.
Click here for our factsheet on quadrivalent and trivalent influenza vaccine options for 2026.
Egg-based and cell-based flu vaccines sometimes use slightly different viruses due to how well the virus replicates in eggs or cells. Even though these viruses may differ, their antigenic properties and how they stimulate the immune system are similar, providing the same protection. You only need one vaccine because both types protect against the same flu strains.
Production of 2026 influenza vaccines
All four available influenza vaccines contain haemagglutinin proteins from the surface of the influenza virus. These proteins are harvested and purified from an influenza virus that is either grown in embryonated chicken eggs (egg-based vaccine) or propagated in Madin Darby Canine Kidney (MDCK) cells (cell-based vaccine, Flucelvax). Four virus strains are produced separately and combined to make the quadrivalent formulation. The adjuvanted formulation, Fluad, also contains a squalene-based oil-in-water emulsion adjuvant, MF59, to stimulate a stronger immune response in older people.
Egg-based vs cell-based vaccines
Egg-based and cell-based vaccines differ in their method of manufacture. Egg-based vaccines are traditionally manufactured by cultivating influenza viruses in embryonated chicken eggs. Once the influenza viruses have replicated in the eggs, the viral particles are harvested, purified and inactivated for use in vaccines. In comparison, cell-based vaccine manufacture uses mammalian cell cultures to propagate the influenza virus.
Replication via cell-line eliminates the requirement for chicken eggs. This can be advantageous in scenarios where egg-based production faces challenges, such as a shortage of eggs, egg adaptation or poor antigenic match due to mutations occurring in the circulating seasonal influenza virus during production. Egg adaptation is a phenomenon in which the virus can undergo genetic mutations as it adapts to growing in the egg environment. This can potentially impact the accuracy of the vaccine to match the circulating influenza strains.
Some studies, comparing the relative efficacy of egg-based and cell-based vaccines, show that cell-based influenza vaccine advantage is more significant during seasons when the variations between the egg-based vaccine strains and the influenza strains circulating in the population are substantial.
Click here for our factsheet on cell-based vaccines. Or to learn more about adjuvanted vaccines, click here.
Standard influenza vaccine effectiveness

For a list of studies and more estimates of inactivated influenza vaccine efficacy and effectiveness per population group (i.e, healthy adults, adults with high-risk conditions, older adults, children etc) look in the Immunisation handbook.
Operational guidance for the 2026 Influenza Programme
Operational guidance including ordering and claiming follows a similar process to 2025.
Refund for unused/expired funded influenza vaccine
Please ensure you continue to have influenza vaccine stock available until 31 December for those who are eligible for influenza vaccination. One refund will be available for a total of 10 doses of unused Influvac Tetra. To be eligible for a refund, the unused stock must be returned prior to 31 January 2027. Email Healthcare Logistics flu@healthcarelogistics.co.nz to request a Return Authorisation.
Responses to vaccine
Responses associated with Influvac Tetra:
- Mild pain, redness and swelling around injection site (children and adults)
- Fever, irritability, loss of appetite (children)
- Headache, muscle aches, fatigue (adults)
Responses associated with Fluad in older adults:
- Warmth, mild pain, swelling, and itching around injection site
- Fatigue, feverishness, nausea, muscle aches, headache
Other formulations and brands
2026 influenza vaccines
There are four influenza vaccines for 2026.
Brands: Influvac Tetra, Flucelvax, Fluad, Fluzone.
Influvac Tetra and Fluzone are inactivated influenza vaccine, split virion, egg-based vaccines.
Flucelvax is an inactivated subunit influenza vaccine, cell culture-based vaccine.
Fluad is an inactivated influenza vaccine, surface antigen, adjuvanted, egg-based vaccine.

Schedule and administration

Schedule vaccines
- Influvac Tetra is the funded influenza vaccine for 2026, for 6 months of age and over.
- Flucelvax and Fluzone are unfunded vaccines, for 6 months of age and over.
- Fluad is an unfunded vaccine, for 50 years and over.
- For ages 6 months to 3 years (inclusive), if an influenza vaccine is being administered for the first time a second dose is required at least four weeks later, for all others a single dose is required. Children under 4 years of age who are receiving influenza vaccine for the first time have a better immune response after two priming doses of the influenza vaccine. For eligible children who required two doses of the vaccine, both doses are funded.
Preparation and Administration
Preparation
Influvac Tetra - shake contents before use
Flucelvax - shake before use
Fluad - shake gently before use
Fluzone - shake well before use
All the influenza vaccines are delivered as a single 0.5mL dose.
Influvac Tetra comes with an attached 16mm needle. In this instance there is no concern with using a smaller length needle in larger arms. The datasheet allows for both IM and SC administration. We do recommend a 90-degree angle unless patient has a medical condition where an angled approach is more appropriate.
Pre-vaccination screening, informed consent, and post-vaccination information
A comprehensive pre-vaccination screening must be completed with the vaccine recipient prior to consent. The IMAC pre-vaccination screening tool can be found here.
The consumer handout What you need to know about the flu vaccination (HP8682) is available to assist with pre-vaccination screening and to provide post-vaccination information. If written consent is required, the 2026 flu vaccine consent form (HP7990) can be used.
Waiting after receiving a 2026 influenza vaccination
Standard post-vaccination wait time is now 15 minutes across all vaccines in Aotearoa, with a possible reduction of the observation period to five minutes*, or an extension of the observation period if it is felt to be appropriate. Wait times can be increased or decreased onan individual basis as deemed appropriate by the vaccinator.
A reduced observation period may be considered for individuals who meet all of the following criteria:
- do not have a history of severe allergic reactions
- have been assessed for any immediate post vaccination adverse reactions (5 minutes)
- know when and how to seek post-vaccination advice
- will have another adolescent or adult with them for the first 15 minutes post-vaccination
- will not drive, skate, scoot, ride a bike or operate machinery until 15 minutes post-vaccination
- have the ability to contact emergency services if required
Click here to refer to the IMAC factsheet, 'Guidelines for post-vaccination wait times'
Special considerations
Egg allergy
Influvac Tetra, Flucelvax, Fluad and Fluzone can be given to people with an egg allergy or a known history of egg anaphylaxis.
See Vaccine Safety page below for more information and other more common situations that may arise during pre-vaccination screening.
Pregnancy
One dose of Influvac Tetra, the inactivated quadrivalent influenza vaccine is recommended and funded each influenza season at any stage of pregnancy through to 31 December 2026. Influenza vaccination provides direct protection from the complications of influenza, both during pregnancy and postpartum. The newborn is also protected through passive immunity for the first few months of life.
For more information see page 19 of the 'Winter Preparedness Kit: Vaccination for Flu, COVID-19 and other respiratory viruses' for more pregnancy-specific info and click here for a detailed factsheet on influenza and vaccination during pregnancy.
Flucelvax and Fluzone are both listed as a Category A for use in pregnancy, so if a consumer wishes to have an alternative non-funded influenza vaccine in pregnancy then they can proceed with any of the listed alternatives (excluding Fluad).
Children
Influenza infection rates are generally highest in children. Vaccination of children can help provide additional protection to those around them, particularly for babies and older people living in the same house. Click here for a detailed factsheet on influenza and vaccination for children.
Older people
Influvac Tetra is funded for those over 65 years. Increasing the number of older people vaccinated against influenza annually can have a significant impact on improving health outcomes in older people, especially in the context of ongoing co-circulation of other respiratory diseases, such as COVID-19 and RSV.
The factsheet, Influenza and vaccination for older people, can be found here, and for more information on adjuvanted vaccines in this population click here.
Māori and Pacific peoples
Māori and Pacific people are at greater risk of developing underlying health conditions, such as cardiovascular disease and chronic respiratory disease, at a younger age than other ethnicities, which increases the risk of severe influenza and complications. Influenza vaccination is recommended.
Mental health
Individuals with mental health disorders are at an increased risk of comorbid health conditions that predispose them to severe complications associated with influenza disease. Influvac Tetra is funded for people under 65 years of age who have serious mental health conditions or are currently accessing secondary or tertiary mental health and addiction services.
Immunocompromised
Individuals who are immunocompromised due to treatment or underlying conditions are at high risk of severe influenza and complications. It is important to offer vaccination prior to the initiation of chemotherapy or immunosuppressive therapy. When this is not possible, influenza vaccination is recommended and can be given whilst receiving most treatments.
Healthcare workers
The WHO and Health New Zealand recommend that healthcare workers are a priority group for influenza vaccination, not only for their own protection by also to reduce the spread of influenza to vulnerable patients, including those who are pregnant.
Number of influenza vaccine doses required
Most people require only one dose of influenza vaccine each year for protection, especially against severe disease, and additional doses generally provide no significant added benefit.
However, the following groups are recommended to receive 2 does of influenza vaccine (4 weeks apart) during the influenza season:
- Children under 4 getting their first flu vaccination
- First-time vaccination post-stem cell, organ transplant or CAR-T cell therapy
A second dose may also be appropriate:
- In pregnancy if a dose as received early in the influenza season prior to becoming pregnant
- Before northern hemisphere travel
Spacing with other vaccines
National Immunisation Schedule vaccines: can all be given at the same time as any influenza vaccine, preferably in a different limb.
Note: Individuals (or parents/legal guardians/power of attorneys) should be informed of the small risk of febrile convulsions in concomitant delivery of PVC13 and influenza vaccines in children aged 6 months to under 5 years. If the individual has a history of febrile convulsions, separation of these vaccines by two days can be offered but is not essential.
When administering Fluad with other adjuvanted vaccines - e.g., Shingrix - consumers should be informed of the possibility of a stronger post-vaccination response when two or more of these are administered together.
Individuals with thrombocytopenia and coagulation disorders
The vaccine can be given intramuscularly (IM) to individuals with stabilised thrombocytopenia, bleeding disorders and to those who are on anticoagulant therapy. The risk of a haematoma should be included as part of the informed consent process.
After vaccination, apply firm pressure over the injection site without rubbing for 10 minutes to reduce the risk of bruising.
Travel
Influenza vaccination is recommended for those planning to travel internationally, including within the Pacific region. If it is getting close to 6 months since their last influenza vaccination, vaccination is recommended prior to travel. Note that any second vaccination is not funded.
Storage
The influenza programme and winter season places increased demand on vaccine providers, refrigerators and stock management, increasing the risk of cold chain breaches and excursions. We strongly encourage all providers complete the checklist linked here before ordering vaccines to ensure they are well-prepared. In addition to the checklist, it is recommended to complete a Cold Chain Accreditation self-assessment.
All influenza vaccines are marked with an expiry date that must be checked before vaccine administration. The expiry date of the vaccine is the last day of the month in the year indicated on the packaging.
Influenza vaccines must always be stored as per the cold chain between +2°C and +8°C, including for off-site vaccinations. Protect from light.
Refer to the National Standards for Vaccine Storage and Transportation for Immunisation Providers 2017 (2nd Edition).
Sites should ensure their Cold Chain Policy is up to date (including contact details for immunisation coordinators) and Cold Chain Accreditation is current. If off-site vaccination is to be offered, the Cold Chain Accreditation must specifically include this.
Vaccine Safety
The influenza vaccines currently used in New Zealand are inactivated. They do not contain live viruses and cannot cause influenza.
Influenza vaccine is generally well tolerated. Some systemic responses to vaccination may appear influenza-like. Common responses associated with the non-adjuvanted influenza vaccines (Influvac Tetra) in children and adults include pain, redness, and/or swelling at the site of injection. Local responses are almost always mild. Systemic responses such as headache, muscle aches and fatigue may occur in adults. Fever, irritability, and loss of appetite are more likely to occur in children. These are generally mild and usually resolve after a day or so. Systemic events may appear influenza-like.
Fever is a common adverse event in children after vaccination. Convulsions associated with fever can occur in susceptible children. Around 3–8 children in 100 aged under 7 years will experience a febrile convulsion, most likely when aged between 16 and 30 months.
Adults aged 50 years or older are more likely to experience local and/or systemic responses to the adjuvanted influenza vaccine, Fluad than the non-adjuvanted Influvac Tetra vaccine because the adjuvant enhances the person’s immune response.
The most significant serious adverse event associated with influenza vaccination is anaphylaxis, a serious allergic response that usually comes on within minutes of receiving the vaccine. This occurs around once in a million influenza vaccine doses.
Vaccine-related serious adverse events, such as a convulsion associated with fever or cellulitis-like local reaction, are rare.
Contraindications and precautions for influenza vaccine
Influenza vaccination is contraindicated for individuals who have had documented anaphylaxis to any ingredient in the vaccine (with the exception of egg allergies - see below) or to a previous dose of inactivated influenza vaccine. These individuals should not receive the vaccine.
Other considerations
Immunocompromised
Individuals who are immunocompromised can receive an influenza vaccination. Those who are immunocompromised are at high risk of severe influenza and complications. If possible, offer vaccination prior to the initiation of chemotherapy or immune suppressant medication. When this is not possible, influenza vaccination can be given while an individual is receiving most treatments. Following cessation of chemotherapy, normal immune responses return after about 30 days. Specialist’s advice should be sought when considering influenza vaccination of individuals who have received a haematopoietic stem cell or solid organ transplantation in the preceding 6 months.
The response to influenza vaccination in those with a poorly functioning immune system is likely to be low; additional preventative strategies are important to reduce their exposure to influenza. It is advisable for all close contacts of immunocompromised people, aged from 6 months, to also receive an influenza vaccine (unfunded).
Egg allergy or egg anaphylaxis
Influvac Tetra, Fluad and Fluzone are egg-based vaccines, but can be administered to people with a history of egg allergy or egg anaphylaxis. Studies have shown that influenza vaccines containing one microgram or less of ovalbumin do not trigger anaphylaxis in sensitive individuals. Each dose of Influvac Tetra, Fluad and Fluzone contains less than one microgram of ovalbumin.
Flucelvax does not contain ovalbumin, as eggs are not used in the manufacturing process.
Seafood, shellfish or other food allergy or anaphylaxis
People with a seafood or shellfish allergy or anaphylaxis can receive an influenza vaccine, including Fluad that contains the MF59 adjuvant derived from shark liver.
Allergy or anaphylaxis to other foods or products are not a contraindication for influenza vaccination.
Sulfonamide (sulphur) allergy
Influvac Tetra, Flucelvax Quad, Fluad Quad, FluQuadri or Alfuria Quad can be given to people with a sulfonamide (sulphur) allergy.
Sulfonamide (sulphur) antibiotics, such as co-trimoxazole, sulfasalazine, and sulphite preservatives used in food, are different to medicines containing the words sulfate or sulphate, (eg, neomycin sulphate). Sulfate itself does not cause allergic reactions. It is safe to use a sulfate when a person has a sulfonamide allergy or a sulfite intolerance.
Antibiotics
Influvac Tetra contains traces of gentamicin and tylosine tartrate. Fluad contains traces of kanamycin and neomycin. The vaccines are contraindicated in people with known anaphylaxis to these respective antibiotics.
No antibiotics are used to manufacture Flucelvax or Fluzone.
History of Guillain–Barré syndrome (GBS)
No association was found between administering a million doses of influenza vaccine and GBS in adults aged from 65 years in the US. The risk of developing GBS is increased following influenza infection, and the magnitude of the risk is several times greater than that possibly occurring following influenza vaccination.
If GBS has occurred within 6 weeks of previous influenza vaccination, the decision to give an influenza vaccine should be based on careful consideration of the potential benefits and risks.
Reporting adverse events following influenza vaccination
Healthcare professionals and vaccinators are professionally and ethically responsible for reporting any serious or unexpected adverse events after the administration of all medicines, including the influenza vaccine, regardless of whether or not they consider the event to have been caused by the vaccination. CARM Reports can be completed online here.
Vaccine Effectiveness
Influenza immunisation protects around 7–8 pregnant women out of 10 from serious influenza related illness requiring hospital treatment. Around half of infants whose mother had an influenza immunisation during pregnancy are also protected from influenza for up to 6 months after birth.
Very little information on how effective the influenza vaccine in infants under 2 years of age has been collected. The information collected suggests about 6–7 in 10infants in this age group will be protected from influenza.
Influenza immunisation will protect around 6–7 in 10 healthy children under 3 years of age, around 6–7 in 10 healthy children under 16 years of age, and 4–6 in 10healthy adults from influenza. The influenza vaccine only has a modest reduction in the time healthy adults take off work due to influenza.
The influenza vaccines have a modest effect, around up to 60%, in preventing confirmed influenza in those aged 65 years and over living in the community and can reduce the number of older people needing to be hospitalised with influenza-related pneumonia and complications. Influenza vaccine has also been shown to reduce the risk of influenza-related pneumonia in older people living in long term care facilities who develop complications related to influenza.
The Institute of Environmental Science and Research (ESR) reported in late 2023, the estimated crude vaccine effectiveness for the preceding flu season (2023) was 80.4% and 58.6% for influenza-confirmed ARI cases and severe acute respiratory illness (SARI) cases, respectively.
Preliminary data from ESR suggests that influenza activity in2023 was described at a low-to-moderate level. Influenza-associated SARI hospitalisations were higher in both young children (aged 0–4 years) and the elderly (above 65 years), compared to other age groups, and higher in Pacific peoples and Māori ethnic groups.
Adjuvanted influenza vaccines
The urgent need for more effective influenza vaccines in the elderly population arises from unique challenges and vulnerabilities associated with ageing. A natural decline in the immune system’s effectiveness is a phenomenon known as immunosenescence. This age-related weakening of the immune response makes older people more susceptible to infections, such as influenza.
Due to immunosenescence, older people are also associated with a heightened risk of influenza-related complications. People aged 65 years or older are at a higher risk for influenza-related mortality. Research indicates that this age group accounts for 7–8 out of 10 influenza-related deaths and 5–7 out of 10 influenza-related hospitalisations, each flu season.
Adjuvanted influenza vaccines are designed to enhance and prolong the immune response. Adjuvants, such as MF59, are added to a vaccine to boost the body’s immune response and improve the vaccine’s effectiveness, especially for those with compromised or weakened immune systems. The more robust an immune response, the better the protection against influenza viruses for the upcoming flu season.
Studies have found a modest improvement in vaccine effectiveness in those above 65 years for those who have received an adjuvanted influenza vaccine, compared with a standard influenza vaccine.
A recent systematic review examining real-world data found that adjuvanted trivalent influenza vaccines were more effective than standard trivalent and quadrivalent influenza vaccines in reducing influenza-related outcomes in older adults. The relative vaccine effectiveness (rVE) of adjuvanted influenza vaccines ranged from 7.5%to 36.3% against standard influenza vaccines in reducing medical encounters and hospitalisations.
In the interest of reducing uncertainties surrounding variations in single-season vaccine effectiveness estimates, a cohort study estimated the relative effectiveness of trivalent adjuvanted influenza vaccines versus non-adjuvanted trivalent/quadrivalent influenza vaccines in preventing all-cause hospitalisation over 18 consecutive flu seasons. The study found that the adjuvanted vaccine cohort was associated with a 12% lower chance of hospitalisation for older adults.
A study that expands on CDC mathematical modelling to estimate the number of additional influenza-related outcomes averted with adjuvanted versus standard influenza vaccines, found that adjuvanted trivalent influenza vaccines were more effective, preventing twice as many influenza illnesses over three seasons in adults over the age of 65 years. Proportionate decreases were also observed in related healthcare use and complications.
For more information on adjuvanted influenza vaccines, including effectiveness and safety, click here.
Cell-based influenza vaccines
There are no randomised trials comparing the efficacy of egg-based and cell-based vaccines, but a number of other types of trials have been performed.
Some studies have shown that cell-based influenza vaccines, such as Flucelvax, have been more effective at preventing illness or inducing an immune response in comparison to standard egg-based vaccines during certain seasons. Cell-based advantage appears to be more pronounced during seasons where substantial variations exist between the egg-based vaccine strains and the circulating strains in the population.
A recent review evaluating the effectiveness of seasonal cell-based quadrivalent influenza vaccine compared to quadrivalent and trivalent egg-based influenza vaccines found an overall pooled relative vaccine effectiveness (rVE) of 8.4%.
Both egg-based and cell-based influenza vaccines effectively prevent severe disease and hospitalisations. Although certain studies indicate modest improvements for cell-based vaccines, the margin of efficacy against egg-based vaccines fluctuates across seasons.
For more information on cell-based influenza vaccines, including effectiveness and safety, click here.
References
- Airey J, Albano FR, Sawlwin DC, Jones AG, Formica N, Matassa V, et al. Immunogenicity and safety of a quadrivalent inactivated influenza virus vaccine compared with a comparator quadrivalent inactivated influenza vaccine in a pediatric population: A phase 3, randomized noninferiority study. Vaccine. 2017;35(20):2745-52.
- Beyer WEP, McElhaney J, Smith DJ, Monto AS, Nguyen-Van-Tam JS, Osterhaus ADME. Cochrane re-arranged: Support for policies to vaccinate elderly people against influenza. Vaccine. 2013;31(50):6030-3.
- Cowling BJ, Thompson MG, Ng TWY, Fang VJ, Perera RAPM, Leung NHL, et al. Comparative reactogenicity of enhanced influenza vaccines in older adults. J Infect Dis. 2020;222(8):1383-91.
- Darvishian M, van den Heuvel ER, Bissielo A, Castilla J, Cohen C, Englund H, et al. Effectiveness of seasonal influenza vaccination in community-dwelling elderly people: An individual participant data meta-analysis of test-negative design case-control studies. Lancet Respir Med. 2017;5(3):200-11.
- Demicheli V, Jefferson T, Di Pietrantonj C, Ferroni E, Thorning S, Thomas Roger E, et al. Vaccines for preventing influenza in the elderly. Cochrane Database Syst Rev. 2018(2):Art.No.:CD004876.
- Frey SE, Reyes MRA-DL, Reynales H, Bermal NN, Nicolay U, Narasimhan V, et al. Comparison of the safety and immunogenicity of an MF59®-adjuvanted with a non-adjuvanted seasonal influenza vaccine in elderly subjects. Vaccine. 2014;32(39):5027-34.
- Health New Zealand | Te Whatu Ora, Immunisation handbook [Internet]. Available from: https://www.tewhatuora.govt.nz/for-health-professionals/clinical-guidance/immunisation-handbook
- Pellegrini M, Nicolay U, Lindert K, Groth N, Della Cioppa G. MF59-adjuvanted versus non-adjuvanted influenza vaccines: Integrated analysis from a large safety database. Vaccine. 2009;27(49):6959-65.
- Pharmaceutical Management Agency (PHARMAC). Pharmaceutical schedule [Internet]. Wellington: PHARMAC; 2021. Available from: https://schedule.pharmac.govt.nz/ScheduleOnline.php.
- Puig-Barbera J, Diez-Domingo J, Varea AB, Chavarri GS, Rodrigo JAL, Hoyos SP, et al. Effectiveness of MF59™-adjuvanted subunit influenza vaccine in preventing hospitalisations for cardiovascular disease, cerebrovascular disease and pneumonia in the elderly. Vaccine. 2007;25(42):7313-21.
- Statler VA, Albano FR, Airey J, Sawlwin DC, Graves Jones A, Matassa V, et al. Immunogenicity and safety of a quadrivalent inactivated influenza vaccine in children 6–59 months of age: A phase 3, randomized, noninferiority study. Vaccine. 2019;37(2):343-51.



